Mild Curve Less than 20-25º

Non-Surgical Treatments
For mild curves measuring less than 20-25º treatment options may involve a combination of observation and monitoring, and occasional physical therapy recommendations. Your scoliosis specialist will need to determine if the curve is progressing or worsening, or if the curve is stable and unchanging.
Observation & Monitoring
Periodic observation and monitoring is usually the first method of treatment for Scoliosis Curves less than 20-25º .
- You will visit your Scoliosis Specialist every four to six months.
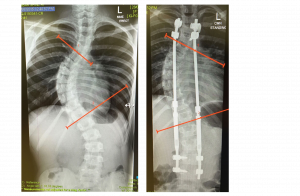
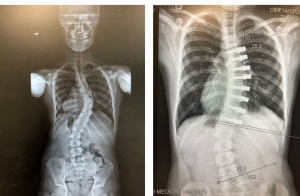
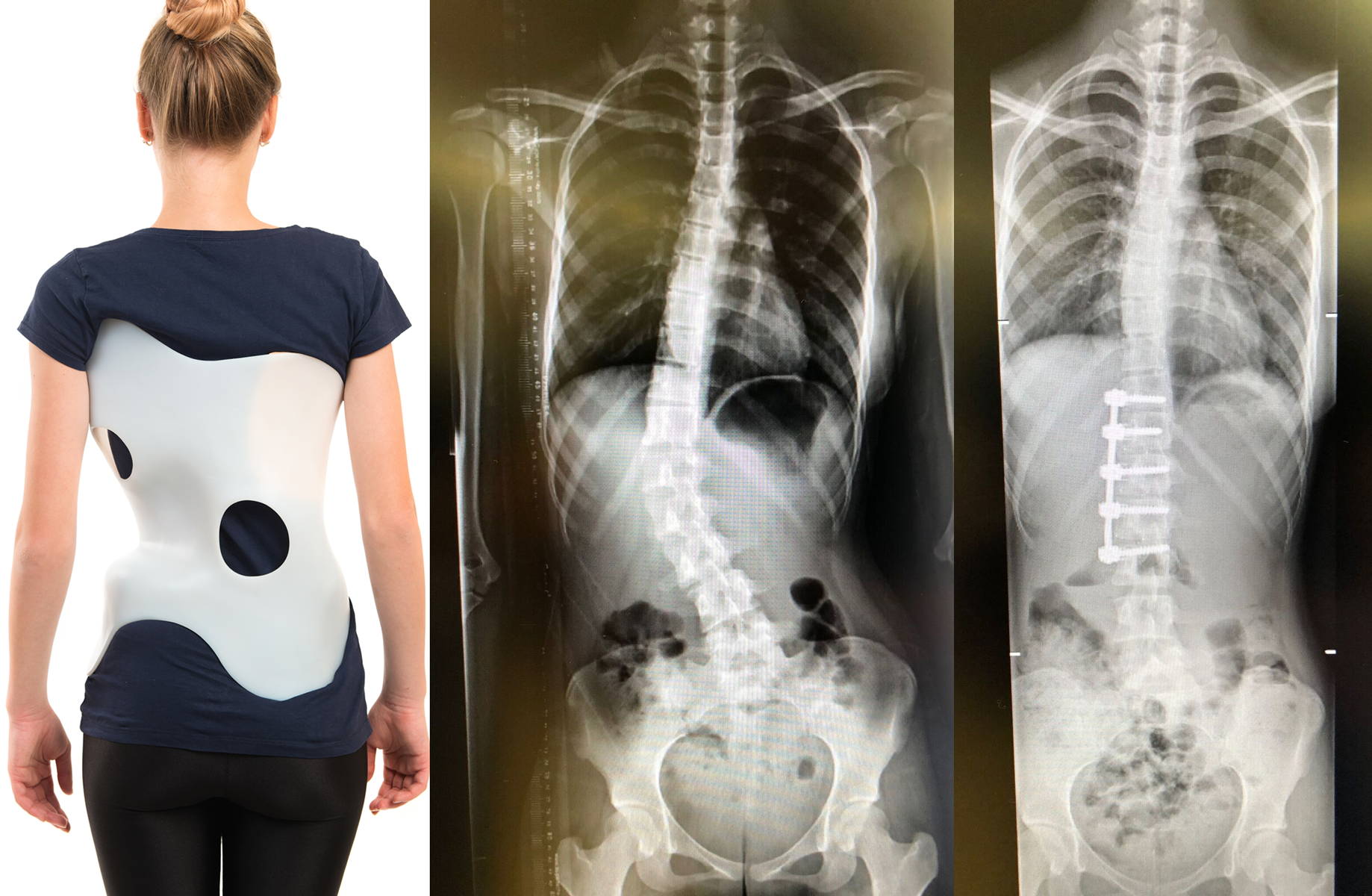
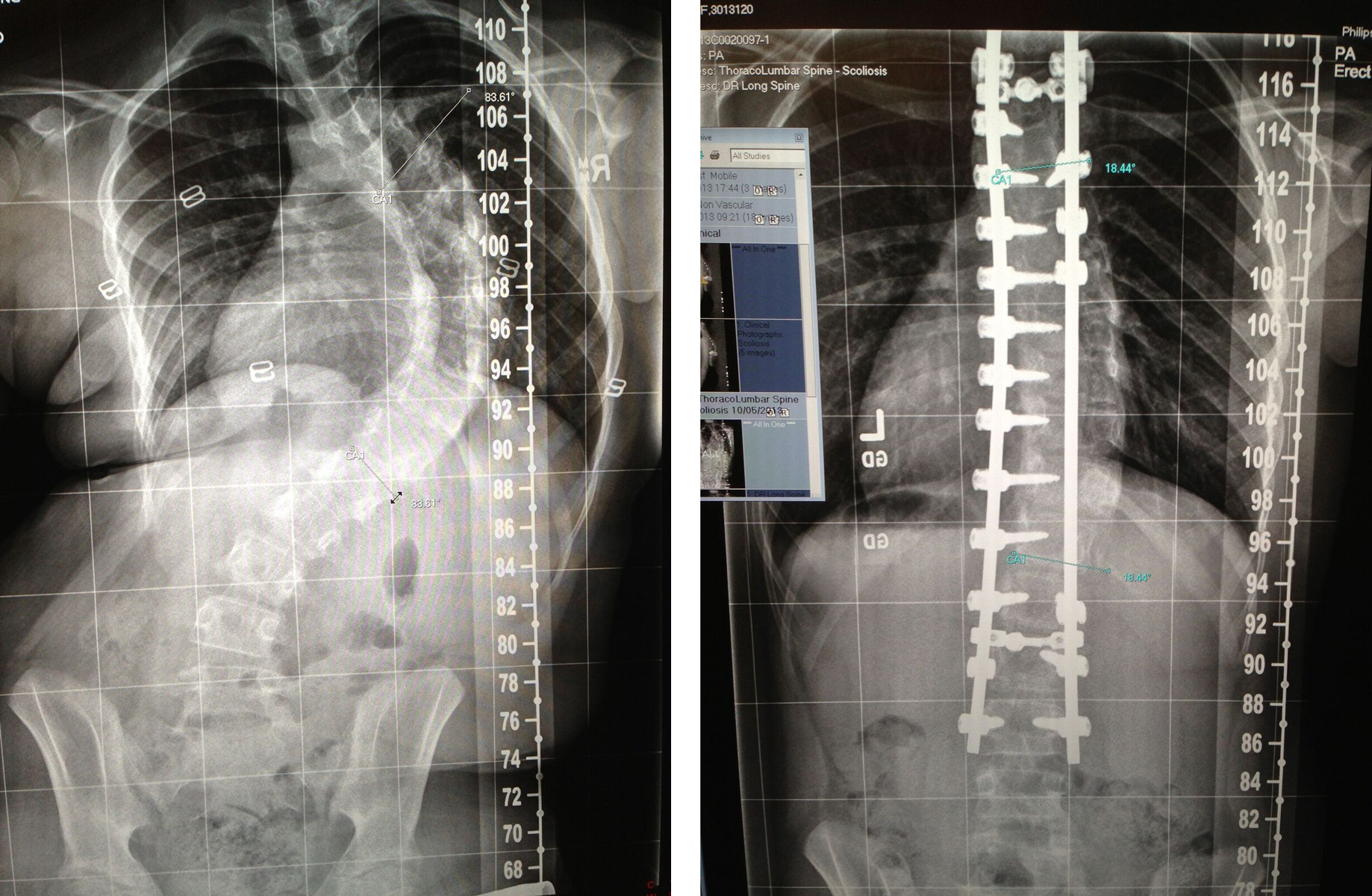
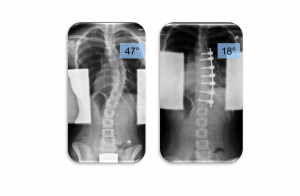
- X-rays or EOS scans will be taken regularly and reviewed against previous films.
- The specialist will document changes and make recommendations for treatments as necessary.
- You may be referred to other specialists to make sure there are no other problems in other parts of the body.
Physical Therapy
Physical therapies may be useful to help strengthen core muscles and manage pain.
Physical therapy (specifically designed – Schroth Method) or some chiropractic therapies have some scientifically proven benefits seen to slow curve progression. They can help strengthen your core muscles, improve general posture and even help manage any discomfort associated in some scoliosis.